The Pancreas
Pancreatic Anatomy
Introduction
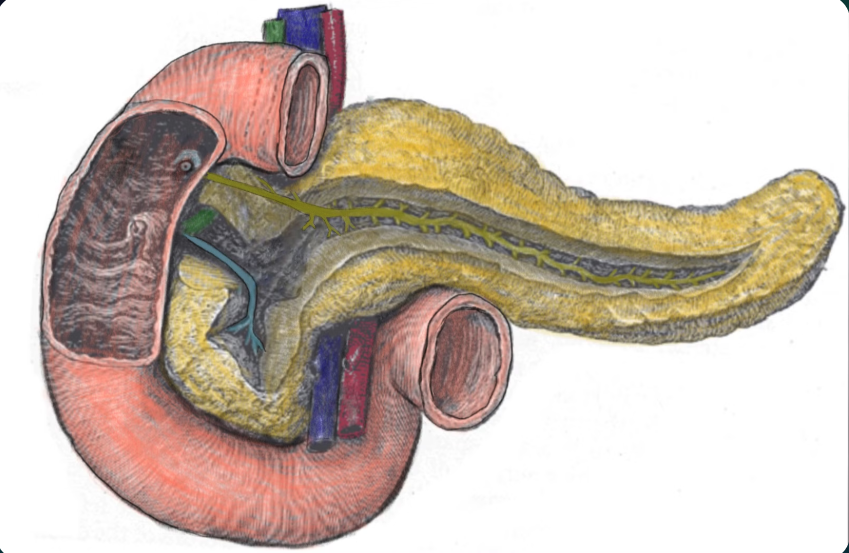
The pancreas is an elongated oblong shaped accessory digestive gland, with endocrine and exocrine functions.
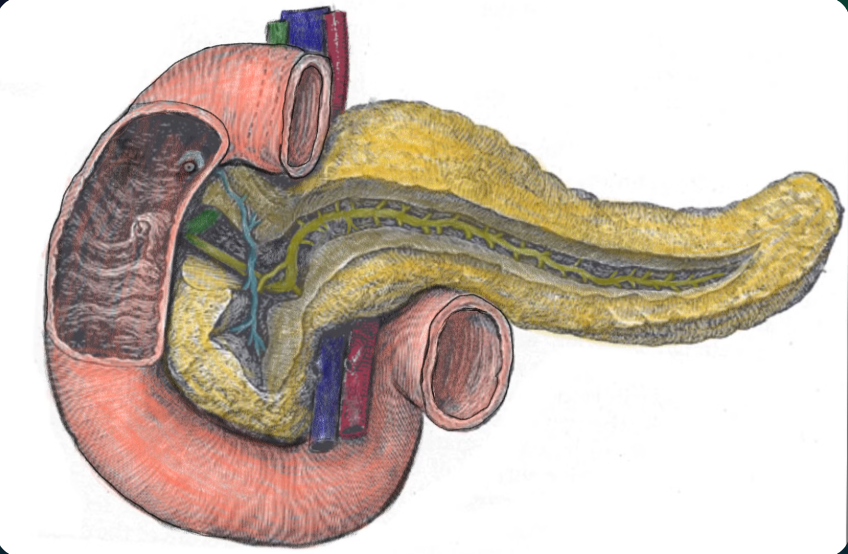
A hand drawing of a pancreas, duodenum and portal triad
Functions Of The Pancreas
Endocrine Function
Related to production of enzymes, performed by Langerhans islets. Hormones produced include:
- Insulin
- Proinsulin
- Amylin
- C-peptide
- Somatostatin
- Pancreatic polypeptide (PP)
- Glucagon
Exocrine function
Intravesical cells produce enzymatic components of pancreatic juice, led into the duodenum through pancreatic ducts. Goblet cells secrete mucus in pancreatic ducts. Composition includes:
- Proteolytic enzymes: trypsin, chemotrypsin, carboxypeptidase
- Lipolytic enzymes: lipase, phospholipase, esterase
- Glycolytic enzymes: lactase, amylase (breaks starch into maltose, maltotriose, and dextrins)
- Nucleolytic enzymes: ribonuclease, deoxyribonuclease (break down nucleic acids into mono- and oligonucleotides)
Parts Of The Pancreas
- The pancreas can be divided into 5 different parts.
- This is done for descriptive purposes (no real boundaries to different parts).
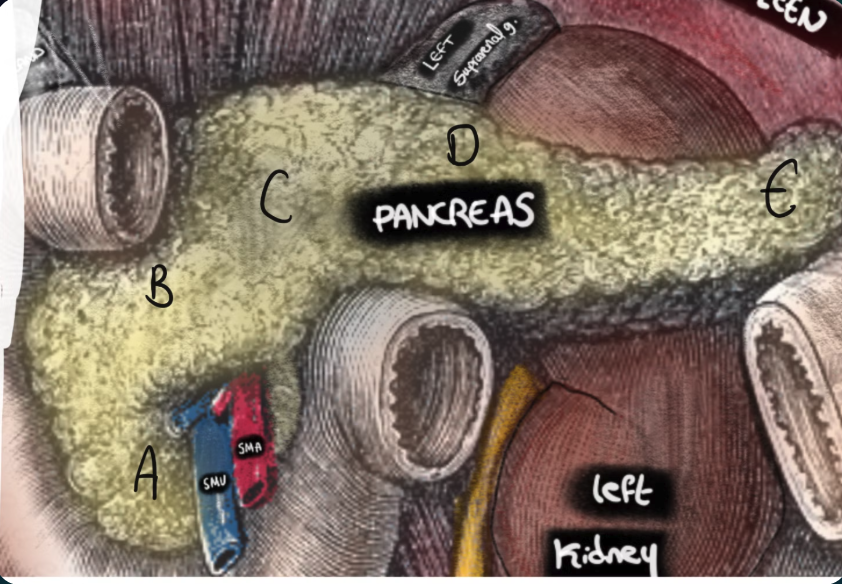
Diagram showing the pancreas divisions labelled A-E
The pancreas divides as follows: (as labelled on the diagram)
Uncinate process
- Projects inferiorly from the pancreatic head.
- Sits behind the superior mesenteric vessels
Head of pancreas
- Part of the pancreas sitting in the C shaped groove formed by the pancreas.
- Removed in pancreaticoduodenectomy
- Separate blood supply to rest of pancreas
Neck of pancreas
- Sits between the head and the body (you don’t say?!)
- Sits anterior to the mesenteric vessels.
- Sits anteriorly to the origin of the portal vein (formed by union of Splenic vein and SMV)
Body of the pancreas
- Continues from the neck
- Lies anterior to the splenic vein
Tail of the pancreas
- An extension of the body
- Closely related to the hilum of the spleen and the left colic flexure
Anatomical Position
- The pancreas lies retroperitoneally (except for the tail) and sits transversally across the posterior abdominal wall.
- It is positioned at the level of the transpyloric plane (L1)
- The pancreas is closely related to a number of vessels described below
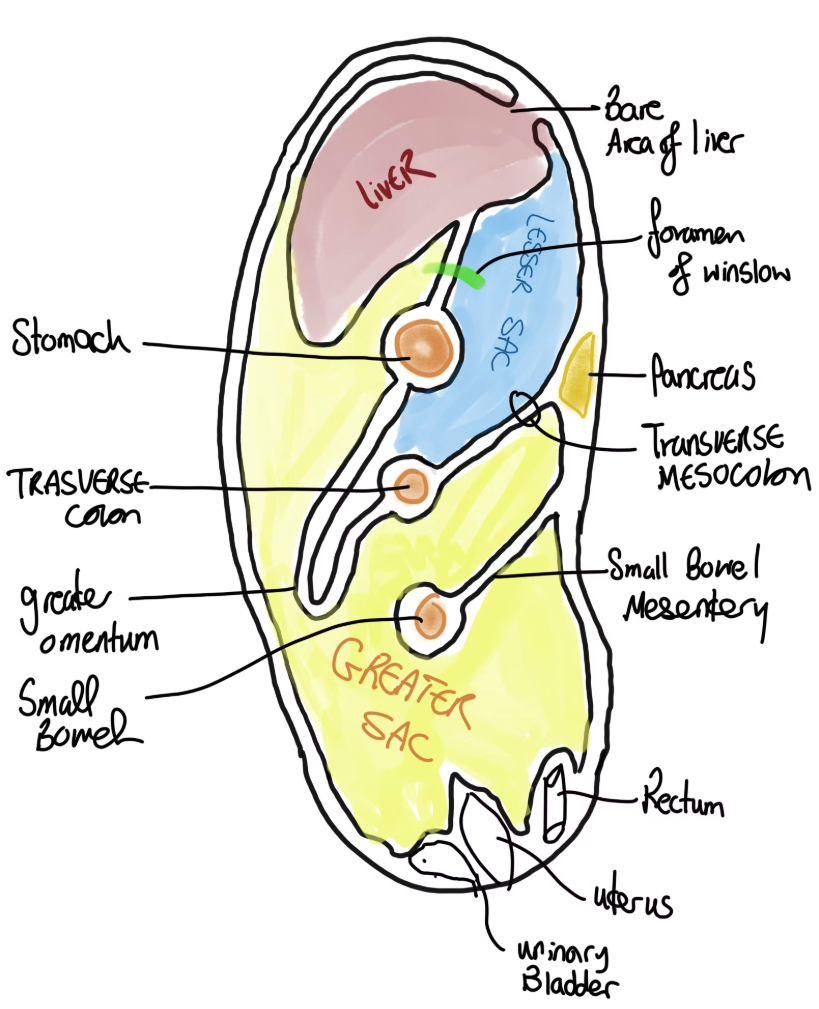
Hand drawn diagram showing sagittal view of an abdomen, depicting anatomical relations of pancreas to the lesser sac and peritoneum
Relation To The SMA
- The Superior Mesenteric Artery (SMA) originates from the abdominal aorta at the level of L1 vertebra
- It runs posterior to the pancreatic neck
- The SMA continues distally, emerging from behind the pancreatic neck
- After emerging, it runs anterior to the uncinate process of the pancreas
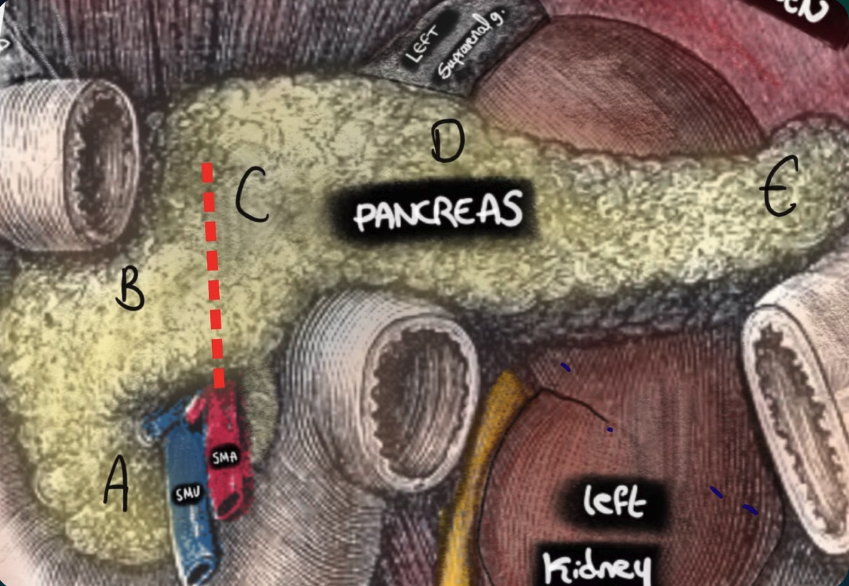
Image showing the relation of SMA to the pancreas. Note the SMA running behind the pancreatic neck and in front of the uncinate of pancreas
Relation to SMV, splenic vein and portal vein
- The splenic vein
- Runs posterior to the pancreatic body
- Is joined by the inferior mesenteric vein behind the pancreatic body
- The SMV
- Drains the right side of the colon and small bowel
- Runs superiorly towards the pancreas
- Will run anterior to the uncinate process (same as SMA)
- Will then lie posterior to the pancreatic neck (same as SMA)
- At this point it joins the splenic vein forming the portal vein
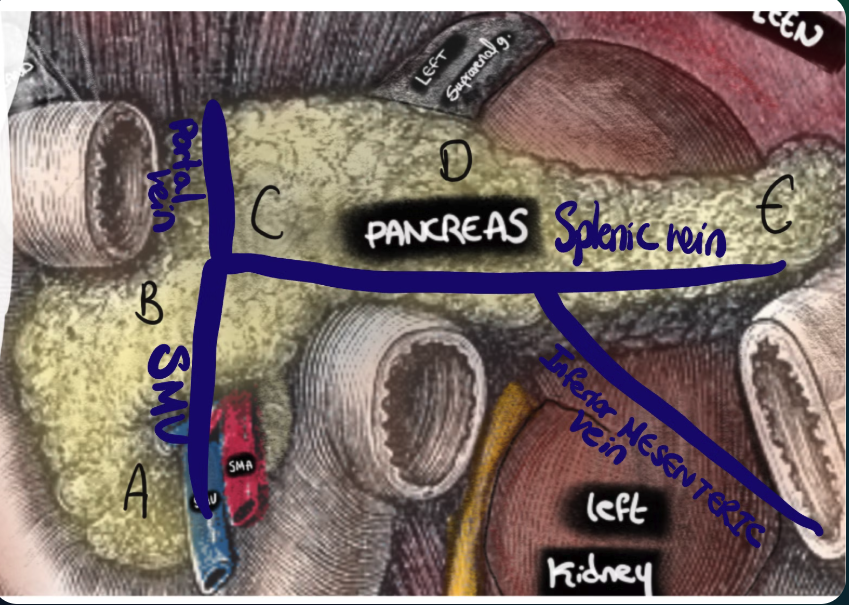
A diagram depicting the relation of the pancreas to the portal vein, and formation of the portal vein from the joining of the SMV and the splenic vein
Relation Of Renal Vein
The renal vein runs anterior to the head of pancreas.
Relations To Other Organs
- Stomach: Anterior to the pancreas, separated by the lesser sac
- Duodenum: The head of the pancreas sits in the C-shaped curve of the duodenum
- D1: Anterior to the pancreatic head
- D2: Lateral to the pancreatic head, to the right
- D3: Sits inferior to the pancreatic head
- D4: In the groove formed by the thinner pancreatic neck
- Transverse Mesocolon: A layer of the greater omentum attaches to the anterior surface of the pancreas
- Peritoneum: No peritoneum behind the pancreas (retroperitoneal)
- Common bile duct: Refer to the ducts section below
- Spleen:
- Anterolateral to the pancreatic tail
- Connected to the tail by the lienorenal ligament
Hand drawn diagram showing sagittal view of an abdomen, depicting anatomical relations of pancreas to the lesser sac and peritoneum
Ductal system:
- 85% of the pancreatic mass is made up of exocrine cells.
- Exocrine tissue drains via multiple small ducts that join to form the main pancreatic duct.
- The uncinate process and lower head drain into the accessory pancreatic duct.
- Both ducts eventually drain into the duodenum.
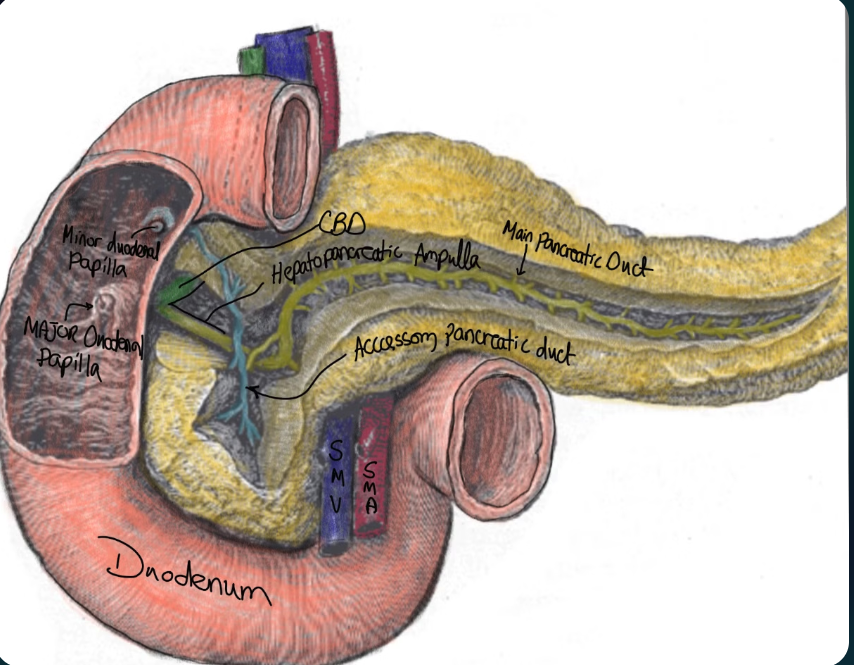
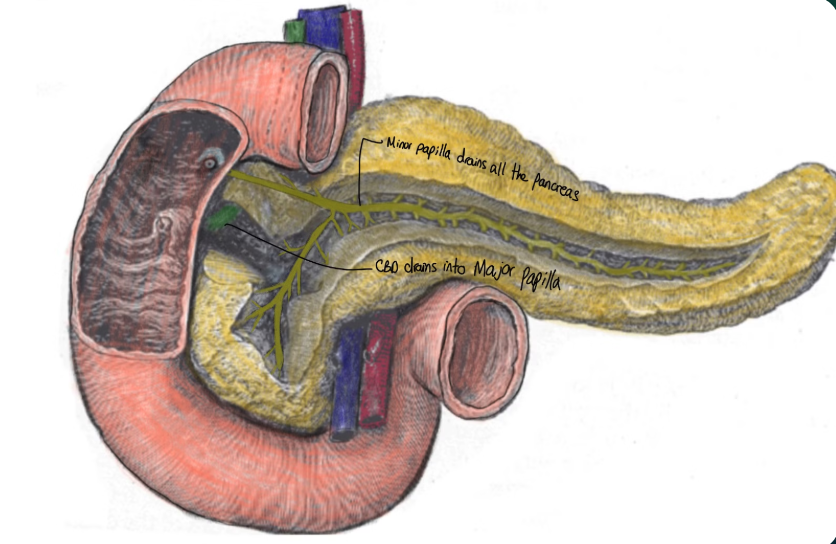
A drawing showing pancreatic duct structures and drainage into the major duodenal papilla
Main Pancreatic Duct (Duct Of Wirsung)
The main pancreatic duct runs from the tail of the pancreas through its center and drains most of the gland. As it nears the duodenum, it joins with the common bile duct at a 60-degree angle to form the hepatopancreatic ampulla. The contents then pass through the sphincter of Oddi and enter the duodenum at the major duodenal papilla.
This papilla is typically located about 7cm distal to the pylorus.
Accessory Pancreatic Duct
- Origin: Derived from the embryological dorsal bud
- Also known as: Duct of Santorini
- Drainage area: Lower part of the head and uncinate process
- Drainage pattern: Partly into the main bile duct and partly into the minor duodenal papilla
Common Bile Duct
The common bile duct (CBD) is closely related to the head of the pancreas. Its configuration can vary:
- Partially covered posteriorly (~50% of cases)
- Completely covered (30% of cases)
- Completely uncovered (16.5% of cases)
- May pass laterally to the pancreatic head (least common)
Variant pancreatic duct anatomy can affect the relationship between the CBD and the pancreas.
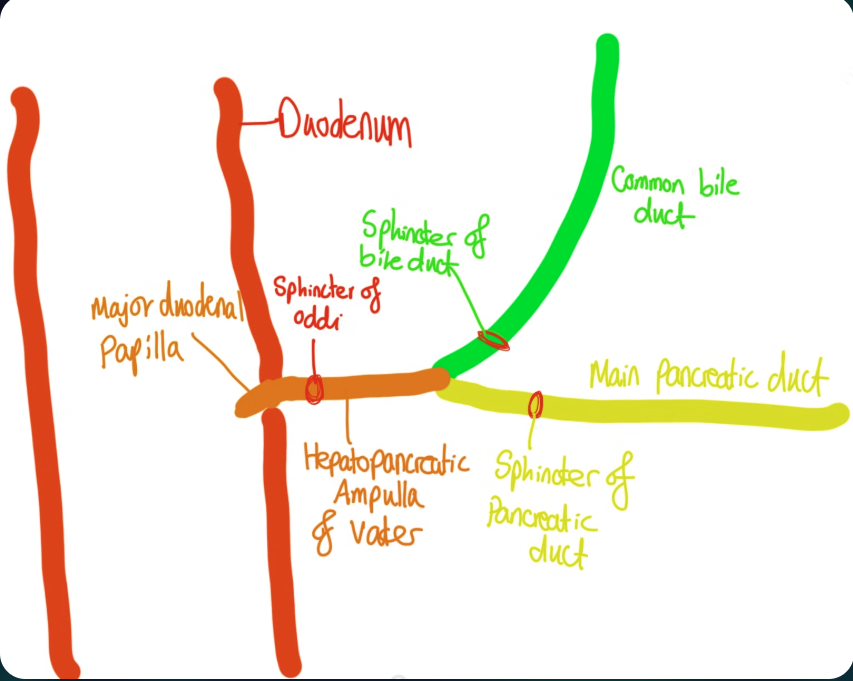
An illustration showing the overall configuration of the pancreatic duct, CBD, and their drainage into the duodenum
Variant anatomy of pancreatic ducts
Pancreatic divisum
- A common congenital abnormality due to failure of fusion between the dorsal and ventral pancreatic ducts.
- Often asymptomatic, but may be linked to recurrent idiopathic pancreatitis.
Subtypes of pancreatic divisum
Type 1 (classic): (COMPLETE DIVISUM) (70% of cases)
- No connection between the two ducts.
- The main duct drains into the minor papilla and the accessory duct into the major papilla.
A diagram showing type 1 pancreatic divisum duct arrangement.
Type 2 (absent ventral duct): (20%)
- The entire pancreas drains via the minor papilla while the CBD drains via the major papilla.
A diagram showing type 2 pancreatic divisum duct arrangement.
Type 3 pancreatic Divisum (around 5%)
- A small or inadequate connection exists between the dorsal and ventral ducts.
Pancreatic Vasculature
Arterial Supply
- Head:
- Superior pancreaticoduodenal artery (branch of the gastroduodenal artery, itself from the celiac axis)
- Inferior pancreaticoduodenal artery (branch of the SMA)
- Body: Pancreatic branches of the splenic artery
- Tail: Supplied by the splenic, gastroepiploic, and dorsal pancreatic arteries
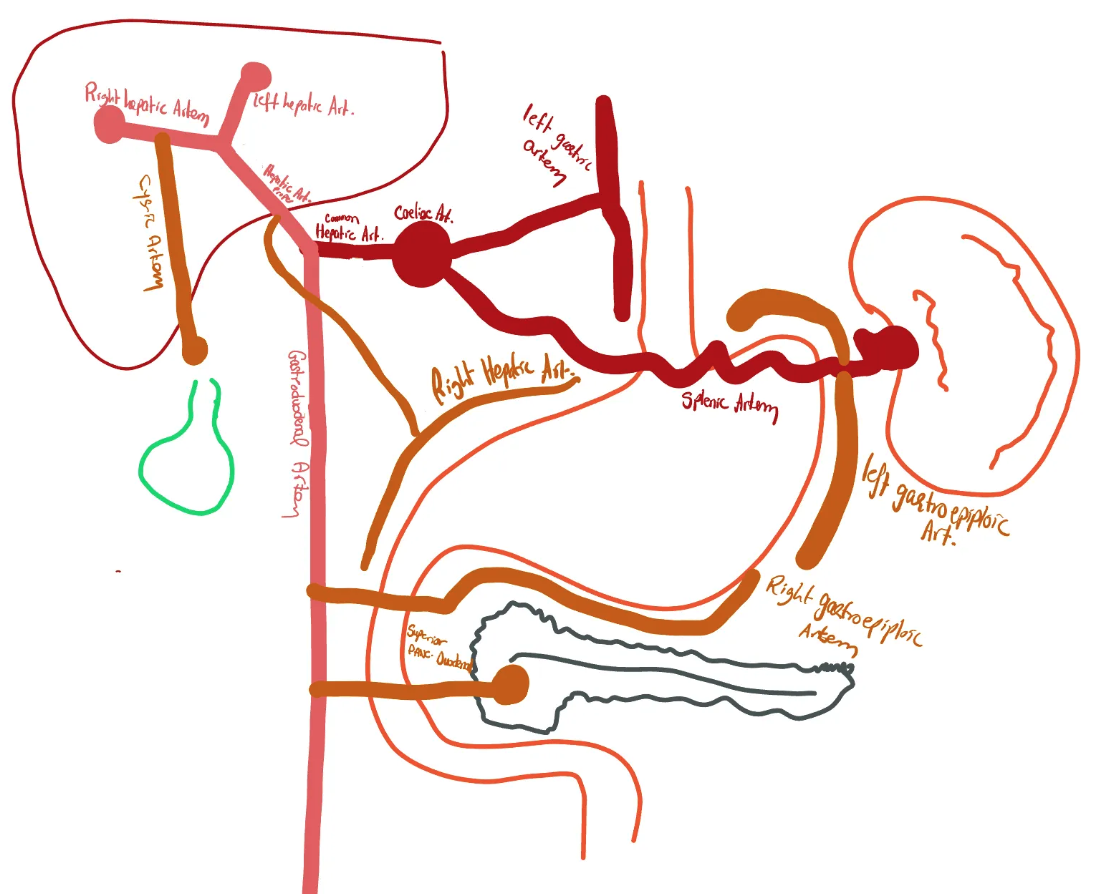
Illustrated diagram showing branches of the celiac axis
Kocherisation Of The Duodenum
Kocherization is the anterior and leftward mobilization of the second part of the duodenum by incising its lateral peritoneal attachments. This maneuver exposes the IVC and left renal vein posteriorly and is used for:
- Whipple’s procedure (pancreaticoduodenectomy)
- Exposing a posterior duodenal perforation
- Exposing the porta hepatis
- Accessing retroperitoneal structures (e.g., aorta in vascular procedures)
It allows medial reflection of the duodenum because the duodenal blood supply comes primarily from its medial aspect.
Steps of Kocherisation
Pre-maneuver Setup:
- Surgeon positioned on the left of the patient
- Liver retracted superiorly (using an assistant or self-retaining retractor)
- Right colic flexure retracted downward
Duodenal Mobilisation:
- Retract the second part of the duodenum to the left
- Incise the lateral fascia
- Mobilize the duodenum and head of the pancreas off the IVC and aorta
- Limit further mobilization by the anteriorly running superior mesenteric vessels
Fascial Layers: The avascular fusion fascia of Treitz allows mobilization since vessels are preserved medially.
Mesoduodenum Restoration: Removal of lateral attachments restores mobility.
Portal Exposure:
- Exposes the porta hepatis
- Allows dissection of the hepatoduodenal ligament
- Provides access to the lesser sac via the foramen of Winslow
Venous Drainage of Pancreas
Venous drainage of head:
Drains into the SMA which then drains into the portal vein.
Venous drainage of body:
Drains via the pancreatic veins into the splenic vein.
Lymphatic Drainage of Pancreas
- Surface and border nodes drain into the celiac and superior mesenteric nodes.
- Upstream drainage continues to the cisterna chyli and thoracic duct.
Nerve Supply
Parasympathetic:
Vagus nerve (CN X)
Sympathetic:
Greater and lesser splanchnic nerves. Sensory nerves accompany the sympathetic fibers.
Select a Clinical Topic
Please choose a specific pathology from the submenu to see the relevant clinical details.
Acute Pancreatitis
Definition
Acute pancreatitis is an acute inflammatory process of the pancreas with varying involvement of local tissues or remote organ systems.
Aetiology:
Most cases can be attributed to one of two causes:
Gallstones
- Three Main Theories of How Gallstones Trigger Pancreatitis:
- Ampullary Obstruction: A gallstone lodges in the ampulla of Vater, blocking pancreatic juice drainage, leading to increased pressure and inflammation.
- Local Inflammation: The stone irritates surrounding tissues, causing inflammation that extends to the pancreas.
- Transient Bile Reflux: Partial obstruction may cause bile to reflux into the pancreatic duct, resulting in irritation and inflammation.
Alcohol Consumption/Excess
The exact mechanism is not fully understood. Hypotheses include:
How Alcohol Affects the Pancreas
Toxic Effects on Pancreatic Cells
Alcohol and its byproducts (e.g., acetaldehyde) directly damage pancreatic acinar cells, leading to oxidative stress, inflammation, and cell death.
Increased Digestive Enzyme Activation
Normally, digestive enzymes are inactive in the pancreas. Alcohol may trigger premature activation, causing the pancreas to digest itself (autodigestion).
Thickened Secretions & Blocked Ducts
Alcohol increases the protein content of pancreatic secretions. This forms plugs that block ducts, leading to backpressure and inflammation.
Increased Sensitivity to Other Triggers
Alcohol weakens the pancreas, making it more susceptible to damage from other factors like a high-fat diet or gallstones.
Changes in Gut-Liver-Pancreas Interaction
Alcohol alters the gut microbiome and increases intestinal permeability, allowing toxins to reach the pancreas and trigger inflammation.
Disruption of Blood Flow
Chronic alcohol use may constrict blood vessels, reducing oxygen supply and predisposing the pancreas to injury.
- Chronic alcohol use may constrict blood vessels, reducing oxygen supply and predisposing the pancreas to injury.
Other Causes of Acute Pancreatitis
Other less common causes can be remembered with the mnemonic: I GET SMASHED
I
Idiopathic
Sometimes no cause is identified.
GET
Gallstones
Gallstones can obstruct the pancreatic duct.
Ethanol
Alcohol-induced pancreatic injury.
Trauma
Blunt abdominal trauma can cause pancreatic injury.
SMASHED
Steroids
Steroid use has been linked to pancreatitis.
Mumps
Approximately 1 in 25 cases of mumps can lead to acute pancreatitis.
Autoimmune
Part of IgG4 related disorders with chronically raised IgG4 levels.
Scorpion stings
A rare cause from the scorpion Tityus Trinitatis.
Hypercalcaemia/Hypertriglyceridaemia
Both have been linked to increased pancreatitis risk.
ERCP
Endoscopic procedures can sometimes trigger pancreatitis.
Drugs
Certain medications can increase the risk of pancreatitis.
Pathophysiology
Trigger to Pancreatitis
- The exact mechanism of pancreatic cell injury remains unclear.
- Local inflammation ensues following the initial insult.
- The inflammatory process may remain local or become systemic.
- Systemic inflammatory cytokines can lead to multi-organ dysfunction.
Clinical Presentation
History
- Patients typically report worsening epigastric pain radiating to the back.
- The pain is often relieved by leaning forward.
- Some patients report prior dull right upper quadrant pain (possibly due to gallstones).
- Nausea and vomiting may occur.
Examination Findings
- Findings range from localized epigastric tenderness to generalized peritonitis.
- In severe cases, signs of cardiovascular or respiratory dysfunction may be present.
- Retroperitoneal bleeding may be evident with:
- Cullen’s Sign: Umbilical bruising.
- Grey Turner’s Sign: Flank bruising.
Diagnosis
How to Diagnose Pancreatitis
- Diagnosis is based on 2 out of 3 criteria:
- Serum amylase/lipase elevation (3x normal or significant rise)
- Characteristic clinical presentation
- CT imaging evidence
A Note on Serum Amylase
- Correlation with clinical and imaging findings is crucial since amylase may be elevated in other conditions:
- Mesenteric infarction
- GI perforation
- Acute cholecystitis
- Diabetic ketoacidosis
- Viral infections
- A normal amylase does not rule out pancreatitis, especially in delayed presentations.
The Use of Serum Lipase
- Lipase is more sensitive and specific than amylase and remains elevated longer.
- Its use may be limited due to cost.
Initial Management of Acute Pancreatitis
- Management is supportive with aggressive fluid resuscitation due to third spacing.
- Monitor vital signs and urine output; involve intensive care if needed.
Severity Scoring
- Severity scoring systems (e.g., Glasgow, Ranson, APACHE II) help predict outcomes.
Glasgow Scoring System
- Cullen’s Sign: Umbilical bruising.
- Grey Turner’s Sign: Flank bruising.
- Serum amylase/lipase elevation (3x normal or significant rise)
- Characteristic clinical presentation
- CT imaging evidence
- Mesenteric infarction
- GI perforation
- Acute cholecystitis
- Diabetic ketoacidosis
- Viral infections
Remember the mnemonic “PANCREAS”:
PANCREAS
PaO2 <8kPa
Indicates respiratory compromise.
Age >55 years
Older patients are at higher risk of severe disease.
Neutrophils (WBC >15×10⁹/L)
High white blood cell count indicates severe inflammation.
Calcium <2mmol/L
Low adjusted calcium signals severe systemic effects.
Renal Function (Urea >16mmol/L)
Indicates significant kidney impairment (AKI).
Enzymes (LDH >600iu/L)
Lactate dehydrogenase elevation suggests tissue damage.
Albumin <32g/L
Low albumin suggests significant fluid leak and inflammation.
Sugar (Glucose >10mmol/L)
Hyperglycemia can indicate beta-cell damage.
Preventing Further Episodes
Look for Gallstones
- Ultrasound is recommended to detect gallstones.
- If negative and suspicion remains, consider EUS or MRCP.
- If gallstones are found, a cholecystectomy should be performed during the same admission if possible.
Alcohol Intake
- Strict cessation of alcohol is the most effective prevention.
Assessment for Other Causes
- If no obvious cause is found, further investigation is warranted.
Supportive Care
Fluid Balance
- Monitor fluid balance rigorously; aggressive IV fluids are required.
- Monitor urine output, blood pressure, and lactate levels.
- Avoid over-resuscitation in patients with cardiopulmonary issues.
Monitoring for Complications
- A CT scan is recommended in patients with prolonged symptoms or biochemical abnormalities.
- CT is ideally performed after 72 hours from symptom onset.
Pain Management
- Effective pain control is critical to prevent respiratory complications.
- PCA may be used in severe cases.
- Avoid NSAIDs to reduce the risk of renal impairment or GI bleeding.
Nutritional Support
- Mild cases: Early oral feeding once nausea subsides.
- Moderate-to-severe cases: Enteral nutrition within 24–48 hours if oral intake is not possible.
- TPN is reserved for cases where enteral feeding is contraindicated.
Complications of Acute Pancreatitis
Systemic Complications
- Acute pancreatitis increases the risk of AKI, ARDS, and distributive shock requiring ICU admission.
Local Complications
Atlanta Classification
Select a classification to see its subtypes and definitions.
Acute Necrotic Collections (ANC)
Occurs in the first 4 weeks; contains a variable amount of fluid and necrotic material; non-encapsulated.
Walled-off Pancreatic Necrosis (WOPN)
Develops after 4 weeks; a mature, encapsulated collection of pancreatic necrosis; has a well-defined inflammatory wall.
Acute Peri-pancreatic Fluid Collection (APFC)
Occurs in the first 4 weeks; homogenous fluid collection confined by normal fascial planes; non-encapsulated.
Pseudocyst
Develops after 4 weeks; a well-circumscribed, encapsulated collection of fluid with a defined inflammatory wall, but no solid necrotic material.

Atlanta classification of pancreatitis complications
Pancreatic Necrosis
What is Pancreatic Necrosis?
- Localized or diffuse non-viable pancreatic tissue due to severe inflammation, ischemia, and autodigestion.
- Necrosis is typically sterile, but infection increases mortality.
- Antibiotic prophylaxis is not recommended unless infection is confirmed.
Which Tissue is Necrotic?
- Parenchymal necrosis: Primarily pancreatic tissue (worse outcomes, ~5%).
- Peripancreatic necrosis: Often associated with better outcomes (~20%).
- Combined necrosis: Most common (~75%).
Infection of Necrotic Tissue
- Two-thirds of necrotic collections remain sterile.
- If infection occurs, mortality increases to 20–30%.
- Indicators include elevated procalcitonin, positive blood cultures, CT guided aspiration, and gas in necrotic tissue.
Diagnosing Pancreatic Necrosis
- CT scan with portal venous contrast is the gold standard.
- MR pancreas can differentiate between solid and liquid necrosis.
Management of Pancreatic Necrosis
- Most sterile necrotic collections resolve with conservative management.
- Intervention is indicated if there is mechanical obstruction or if infected necrosis fails to respond to antibiotics.
Interventions for Pancreatic Necrosis
- Surgical Management:
- Open necrosectomy is the standard approach but carries high mortality (~25%) and fistula risk.
- Laparoscopic necrosectomy may reduce mortality and risk of multi-organ failure.
- Percutaneous Approach:
- Percutaneous drainage under US or CT guidance (preferably retroperitoneal) minimizes complications.
- Success rate is around 55.7% with a mortality rate of 15.4% in infected cases.
- Endoscopic Approach:
- Drainage via puncture through the gastric or enteric wall under ultrasound guidance.
- A stent is placed after tract dilation to allow drainage.
- Mechanical debridement may be performed for more solid necrosis.
- Irrigation (e.g., with hydrogen peroxide) may reduce the need for repeat procedures.
Pancreatic Pseudocyst
What is a Pseudocyst?
- A well-defined collection of pancreatic fluid that appears after 4 weeks of symptom onset.
- Called “pseudo” because it lacks an epithelial lining.
Aetiology of Pseudocysts
- Disruption of the pancreatic duct leads to extravasation of fluid and pseudocyst formation.
Complications of a Pseudocyst
- Haemorrhage: Erosion of nearby vessels can cause life-threatening bleeding; managed via interventional radiology.
- Infection: Can occur spontaneously or post-procedure; treated with antibiotics and drainage.
- Biliary Obstruction: A large cyst in the head may obstruct the CBD, causing jaundice and cholangitis.
- Gastric Outlet Obstruction: Compression of the stomach may cause early satiety or obstruction.
- Portal Hypertension: Compression of splenic or portal veins can increase portal pressure.
Management of Pseudocysts
- Most small pseudocysts resolve spontaneously and require only imaging surveillance.
- Complicated pseudocysts require drainage, usually via a cystogastrostomy.
- Endoscopic stenting (e.g., Hot Axios) is now preferred over open surgery.
- The stent remains in place for at least 6 weeks, and is removed after resolution.
Long Term Complications of Pancreatitis
Endocrine Insufficiency
- Recurrent or severe pancreatitis may destroy beta-cells, resulting in pancreatogenic (Type 3C) diabetes.
- This condition is irreversible.
Exocrine Insufficiency
- Loss of pancreatic tissue can impair enzyme secretion, causing malabsorption and steatorrhea.
- Management involves pancreatic enzyme replacement therapy (PERT) such as Creon.
- Some patients may eventually regain function and wean off PERT.
Pancreatic Cancer
Definition
Pancreatic cancer is a highly aggressive malignancy, most commonly pancreatic ductal adenocarcinoma (PDAC, ~90%). It has a poor prognosis due to late presentation and early metastasis.
Epidemiology
Statistics
- Incidence: ~10-15 per 100,000/year (UK).
- Age: Peak >70 years.
- Sex: Slight male predominance.
- Modifiable: Smoking, obesity, alcohol (via chronic pancreatitis).
- Non-modifiable: Chronic pancreatitis, diabetes mellitus, family history, genetic syndromes (BRCA2, Lynch, Peutz-Jeghers).
Risk factors:
Pathophysiology
- Common mutations:
- KRAS (90-95%) – oncogenic driver.
- TP53 (50-75%) – tumour suppressor loss.
- CDKN2A (p16 inactivation).
- SMAD4 (loss in ~55%) – associated with metastasis.
- Spread:
- Local invasion → Bile duct, duodenum, stomach, nerves (severe pain).
- Lymphatic → Peripancreatic and para-aortic nodes.
- Hematogenous → Liver (most common), lungs, peritoneum.
Clinical Features
Classic Presentation:
- Painless obstructive jaundice (head of pancreas tumours).
- Epigastric pain (body/tail tumours, radiates to back, worse at night).
- Unexplained weight loss & anorexia.
Courvoisier’s Law
If a patient has painless jaundice + a palpable gallbladder, the cause is likely malignant biliary obstruction (e.g., pancreatic cancer).
Diagnosis
- Blood Tests: ↑ ALP, ↑ GGT, ↑ bilirubin, CA 19-9.
- Imaging:
- CT pancreas (triple-phase contrast): Gold standard for diagnosis & staging.
- Endoscopic ultrasound (EUS) + biopsy: Best for histological confirmation.
Histopathology
- Macroscopic: Firm, gritty mass (head of pancreas most common).
- Microscopic:
- Irregular glandular structures in a desmoplastic (fibrotic) stroma.
- Perineural invasion (causes severe pain).
Management
- Surgical:
- Whipple’s procedure (pancreaticoduodenectomy) → For head tumours.
- Distal pancreatectomy → For body/tail tumours.
- Non-Surgical:
- Neoadjuvant chemotherapy: FOLFIRINOX for borderline resectable cases.
- Palliative chemotherapy: FOLFIRINOX or gemcitabine ± nab-paclitaxel.
- Supportive Care: Biliary stenting (ERCP), pain management, enzyme replacement.
Prognosis
- Resectable disease: 5-year survival 15-25%.
- Locally advanced: less than 5%.
- Metastatic: ~1% (median survival 3-6 months).
Key Takeaways
- Painless jaundice + Courvoisier’s sign → Suspect pancreatic cancer.
- CT scan is the gold standard for diagnosis.
- Surgery is the only curative option**, but most present late.
Other Pancreatic Lesions
incidental finding of pancreatic lesions is a common finding on CT or MRI scans. Those lesions classically are classified into solid lesions and cystic lesions. The management of these lesions differ due to some having a malignant potential.
Cystic Lesions
Cystic Lesions of the Pancreas
Select a category to compare benign and pre-malignant lesions.
Pseudocyst (Inflammatory)
Definition: A fluid-filled collection that lacks a true epithelial lining, typically occurring after an episode of pancreatitis.
Key Features: Contains enzyme-rich fluid (high amylase/lipase) and is defined by a fibrous capsule. It is not a true neoplasm.
Malignancy Risk: None.
Management: Drain only if symptomatic (e.g., pain, obstruction).
Serous Cystadenoma (SCA)
Definition: A benign neoplasm composed of glycogen-rich cuboidal epithelial cells, often found in older women.
Key Features: Typically has a microcystic “honeycomb” pattern with clear, serous fluid. Often associated with VHL mutations.
Malignancy Risk: None.
Management: Observe unless the lesion becomes very large and causes symptoms.
Mucinous Cystic Neoplasm (MCN)
Definition: A pre-malignant cystic neoplasm almost exclusively found in the body/tail of the pancreas in women.
Key Features: A thick-walled, mucin-filled cyst that does NOT communicate with the main pancreatic duct. Often has “ovarian-type” stroma.
Malignancy Risk: Yes.
Management: Surgical resection is typically recommended, especially if >4 cm or with high-risk features.
(D) Intraductal Papillary Mucinous Neoplasm (IPMN)
Definition: A pre-malignant, mucin-producing neoplasm that arises within the pancreatic ducts themselves.
Key Features: Characterized by its connection to the pancreatic duct system, causing ductal dilation. Associated with KRAS/GNAS mutations.
Malinancy Risk: Yes.
Management: Surgery is recommended for main-duct IPMN or branch-duct IPMN with high-risk features. Others may be surveyed. This decision is MDT led.
Solid Lesions
Solid Lesions of the Pancreas
Select a category to compare benign and neoplastic solid lesions.
Fibromas & Lipomas
Definition: Extremely rare, true benign soft tissue tumours composed of fibroblasts (fibromas) or adipocytes (lipomas).
Malignancy Risk: None.
Management: No treatment is required unless they grow large enough to cause symptoms by compressing other structures.
Pancreatic Neuroendocrine Tumour (PNET)
Definition: Arises from pancreatic islet cells and can be “functional” (hormone-secreting) or “non-functional”.
Malignancy Risk: Some. Risk is variable depending on size, grade, and functionality.
Management: Surgery is recommended if the PNET is functional or shows malignant features.
(C) Solid Pseudopapillary Tumour (SPT)
Definition: A rare, low-grade malignancy that primarily affects young women. Characterized by a mix of solid and cystic areas.
Malignancy Risk: Low, but present.
Management: Surgical removal is the standard of care and is typically curative.
Whipple’s Procedure (Pancreaticoduodenectomy)
Introduction
- A procedure where the head of pancreas, duodenum, bile duct, gallbladder, part of the stomach is resected.
- Primarily performed to treat head of pancreas cancer and peri-ampullary malignancies/ some benign lesions.
Indications
Malignant Conditions
- Pancreatic head adenocarcinoma (most common)
- Ampullary carcinoma
- Distal cholangiocarcinoma (bile duct cancer)
- Duodenal adenocarcinoma
- Neuroendocrine tumours (e.g., insulinoma, gastrinoma)
Benign Conditions
- Chronic pancreatitis (in selected cases)
- Benign pancreatic head tumours (IPMN, SPT, cystic neoplasms)
- Duodenal trauma (rare indication)
Anatomy Involved
- Pancreas (head, uncinate process)
- Duodenum (first and second parts, sometimes third)
- Common bile duct (distal portion)
- Gallbladder
- Stomach (partial removal in classic Whipple)
- Vascular structures (SMA, SMV, portal vein)
Surgical Procedure
Step 1: Resection
- Kocherisation: Mobilize the duodenum and pancreatic head.
- Division of the bile duct: At or above the level of the cystic duct.
- Resection of the duodenum: Typically including the first and second parts.
- Partial gastrectomy (Classic Whipple) or Pylorus Preservation (PPPD).
- Transection of the pancreas: At the neck, anterior to the SMV.
- Lymphadenectomy: Regional lymph node dissection.
Step 2: Reconstruction
- Pancreaticojejunostomy: Anastomosis of the pancreatic remnant to the jejunum.
- Hepaticojejunostomy: Anastomosis of the common hepatic duct to the jejunum.
- Gastrojejunostomy: To restore gastrointestinal continuity (if a classic Whipple is performed).
Variants of Whipple’s Procedure
- Classic Whipple: Involves partial gastrectomy.
- Pylorus-Preserving Pancreaticoduodenectomy (PPPD): Preserves the pylorus, reducing postoperative dumping syndrome.
Complications
Early Postoperative Complications
- Anastomotic leak
- Leak can occur from any of the three anastomoses:
- Pancreaticojejunostomy (most common)
- Hepaticojejunostomy
- Gastrojejunostomy
- Pancreaticojejunostomy-specific points:
- Occurs in approximately 5–20% of patients.
- Higher risk in:
- Soft pancreatic texture
- Small pancreatic duct (<3 mm); patients with longstanding obstruction may have less risk.
- Inexperienced surgical technique
- Invagination techniques (vs. duct-to-mucosa)
- Clinical Significance:
- Most feared complication of Whipple’s procedure.
- May progress to:
- Postoperative pancreatic fistula (POPF)
- Intra-abdominal sepsis
- Abscess formation
- Haemorrhage:
- Timing:
- Early haemorrhage: Within 24 hours post-op, usually due to technical/surgical issues
- Late haemorrhage: After 24 hours, often due to vessel erosion or infection-related pseudoaneurysm
- Common Sources:
- Gastroduodenal artery stump: Most common site of post-pancreatectomy haemorrhage
- Pancreaticojejunostomy site: From arterial branches or capillary oozing due to leakage and erosion
- Hepatic artery or branches: May be eroded by adjacent collection or leak
- Portal vein or SMV (superior mesenteric vein): Rare but catastrophic if injured or eroded
- Anastomotic bleeds: From gastrojejunostomy or hepaticojejunostomy staple/suture lines
- Pseudoaneurysm rupture: Secondary to infection or pancreatic fistula; often involves the GDA stump or hepatic artery
- Clinical Signs:
- Drop in haemoglobin/haematocrit
- Haematemesis or melaena (if intraluminal)
- Drain output turning haemorrhagic (if extraluminal)
- Hypotension and shock (in severe cases)
- Management:
- Stabilisation: IV fluids, blood transfusion, correction of coagulopathy
- Imaging: CT angiography to identify bleeding source
- Intervention:
- Endovascular embolisation (first-line for most arterial bleeds)
- Endoscopy (for luminal bleeds)
- Surgical re-exploration if bleeding is uncontrolled or unstable
- Timing:
- Prevention Strategies:
- Duct-to-mucosa anastomosis for soft glands
- Consider somatostatin analogues (e.g. octreotide)
- Careful preoperative patient selection
- Routine intraoperative drain placement
- Leak can occur from any of the three anastomoses:
- Delayed gastric emptying
- Bile leak
- Haemorrhage: Intra-abdominal, anastomotic, or pseudoaneurysm-related
- Postoperative infections:
- Intra-abdominal abscess
- Wound infection
- Cholangitis
- Pneumonia
Late Complications
- Diabetes mellitus: Due to endocrine pancreatic insufficiency
- Malabsorption and steatorrhea: Due to exocrine pancreatic insufficiency
- Dumping syndrome: Especially if a partial gastrectomy was performed
- Biliary strictures: Leading to jaundice or cholangitis
Prognosis and Survival
- Pancreatic cancer: 5-year survival post-Whipple: 20–25% (higher if early-stage)
- Other periampullary cancers: Generally better prognosis than pancreatic adenocarcinoma
- Benign conditions: Surgery can be curative, but with potential for significant long-term morbidity
Postoperative Management
- Early mobilisation and physiotherapy
- Nutritional support: TPN if needed, gradually reintroduce oral intake
- Pancreatic enzyme replacement therapy (PERT): To manage exocrine insufficiency
- Diabetes management: If endocrine dysfunction occurs
- Surveillance: Monitor for recurrence with CT scans and tumour markers (e.g. CA 19-9)
Choose Your Quiz Type
Knowledge Quiz
Quiz Progress
Question: 1 / 5
Answered: 0
Remaining: 5